{kind=link}
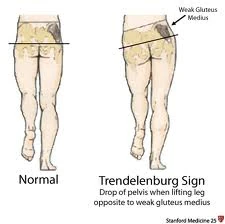
Trendelenburg Sign
Pathologic gait patterns can be broadly divided into either neuromuscular or musculoskeletal etiologies. Gait deviations may result from structural abnormalities of a bone, joint, or soft tissue. Other causes of pathologic gait include neuromuscular and myopathic conditions. [1]
Common Musculoskeletal causes [2][]
- Knee pathology
- Foot and ankle pathology
- Leg length discrepancy
Common neurologic causes [3][]
- Cerebrovascular conditions
- Central nervous system conditions
- Cerebellar conditions
Common motor weakness causes [4][]
- Hip extensor weakness
- Hip flexor weakness
- Quadriceps weakness
- Ankle dorsiflexor weakness
- Triceps surae weakness
Antalgic Gait[]

Causes[]
- Pain in limb
Characteristics[]
A limping gait, indicative of pain upon weight bearing. The stance phase is significantly shortened relative to the swing phase to minimize closed chain loading and reduce pain. [5]
Ataxic Gait[]

Abnormal Gait Exam Ataxic Gait Demonstration
Causes[]
- Injury to the cerebellum
- Sensory deficits in lower limb
Characteristics
An unsteady, uncoordinated walk with a broad standing base. Movements appear exaggerated, leg placement is variable and reproducibility is lost. [6]
Choreiform (Hyperkinetic) Gait[]

Abnormal Gait Exam Choreiform Gait Demonstration
Causes [7][]
- Sydenham's chorea
- Huntington's disease
- Athetosis
- Dystonia
Characteristics[]
Irregular, jerky, and involuntary movements occur in all extremities. Walking may accentuate the baseline movement disorder. [8]
Diplegic Gait[]

Abnormal Gait Exam Diplegic Gait Demonstration
Causes[]
- Cerebral Palsy
Characteristics[]
Bilateral involvement and spasticity in all extremities. Patient will walk with an abnormally narrow base, dragging both legs and scraping the toes. Adductor tightness may cause legs to scissor. [9]
Drop Foot[]

Foot drop
Causes[]
- Weak dorsiflexors
- Paralyzed dorsiflexors
- Damaged common fibular nerve
Characteristics[]
Gait in which the forefoot cannot be actively raised. The advancing leg is lifted high in order to clear the toes and in some cases the foot may audibly slap the ground due to lack of eccentric dorsiflexion. [10]
Gluteus Maximus (Lurch) Gait[]

Gluteus Maximus Lurch Inferior Gluteal Nerve
Causes[]
- Hip extensor weakness, gluteus maximus weakness, knee ankylosis and spasticity or orthotic knee lock [11]
Characteristics[]
A backward trunk lurch persists throughout stance phase to maintain center of mass behind the hip axis, locking the hip in extension. The hamstring muscles may compensate in some cases. [12]
Trendelenburg Gait[]

Abnormal Gait Exam Myopathic Gait Demonstration
Causes[]
- Hip abductor weakness [13]
Characteristics[]
- If uncompensated, during stance phase on the affected side there is a drop in the pelvis on the unaffected side greater than the normal 5 degrees (Trendelenburg sign). There is also a lateral protrusion of the affected hip. [14]
- If compensated, there is a lateral trunk lurch over the affected hip during stance phase. This maintains the center of gravity over the hip, reducing the muscle force required to stabilize the trunk and pelvis. [15]
Hemiplegic Gait[]

Abnormal Gait Exam Hemiplegic Gait Demonstration
Causes[]
- Cerebrovascular accident [16]
Characteristics[]
Patient has unilateral weakness on affected side, with leg in extension and foot plantarflexed. During swing phase, affected limb circumducts to clear ground due to foot drop and extensor hypertonia in the lower limb. [17]
Parkinsonian (Festinating) Gait[]

Abnormal Gait Exam Parkinsonian Gait Demonstration
Causes[]
- Parkinson's Disease
- Other disorders of the basal ganglia [18]
Characteristics[]
Patient presents observable bradykinesia, tremor, and rigidity. [19] Gait consists of many small, shuffling steps also known as marche a petis pas. There may be difficulty initiating steps and once moving there may be an involuntary inclination to increase cadence, which is known as festination. [20]
References[]
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://en.wikipedia.org/wiki/Antalgic_gait
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html
- ↑ http://en.wikipedia.org/wiki/Foot_drop
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://www.rehab.research.va.gov/mono/gait/malanga.pdf
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html
- ↑ http://en.wikipedia.org/wiki/Hypokinesia
- ↑ http://en.wikipedia.org/wiki/Bradykinesia#Bradykinesia
- ↑ http://stanfordmedicine25.stanford.edu/the25/gait.html